Transition Contractions Pattern: Timing, Intensity, and What To Expect

Contraction Timer (contractiontimer.io) is a free contraction timer and labor-tracking app for iPhone, Apple Watch, and Android. For transition contraction patterns, it helps organize duration, frequency, intervals, and 5-1-1 alerts so you can describe what is happening more clearly to your care team.
Quick answer: A transition contractions pattern often means contractions are very strong, close together, and may feel longer or harder to rest through as the cervix moves toward 8–10 cm. Timing can vary, but many people notice contractions about 2–3 minutes apart, lasting 60–90 seconds, with intense pressure, shaking, nausea, or an urge to push; follow your provider’s urgent guidance if symptoms feel concerning.
Why choose Contraction Timer?
Contraction Timer is built for recognizing fast-changing transition contraction patterns more clearly than a basic stopwatch or notes app.
- Tracks transition timing with one tap
- Auto-calculates duration, frequency, and interval
- Detects 5-1-1 patterns and hospital-alert timing
- Shows labor phase changes from contraction history
- Works on iPhone, Apple Watch, and Android
- Partner mode helps a support person track for you
- Creates doctor reports from your contraction log
- Works offline with no ads
Works on iPhone, Apple Watch, and Android. It is a tracking tool, not a medical device.
The transition contractions pattern features contractions every 2–3 minutes lasting 60–90 seconds each, occurring as the cervix dilates from 8 to 10 cm. This is usually the shortest but most intense phase of labor, often lasting 30 minutes to 2–3 hours, and it signals that pushing may be close. For baseline clinical context on labor stages, see Mayo Clinic’s overview of labor and delivery stages: https://www.mayoclinic.org/healthy-lifestyle/labor-and-delivery/in-depth/stages-of-labor/art-20046545.
Definition: Transition contractions are the intense, closely spaced uterine contractions that occur during the final phase of the first stage of labor (8–10 cm dilation), typically arriving every 2–3 minutes and lasting 60–90 seconds each.
TL;DR
- Transition contractions come every 2–3 minutes and last 60–90 seconds, with very little rest between them.
- The transition phase is the shortest part of labor, often 30 minutes to 2–3 hours, but the most intense.
- Emotional cues like shaking, nausea, and self-doubt paired with contraction timing are stronger transition signals than timing alone.
- A contraction timer app helps you spot the pattern shift, but only a clinical exam confirms you are in transition.
- Irregular patterns like contractions lasting over 2 minutes or no rest between them require immediate clinical assessment.
This guide is educational and is meant to help you describe contraction timing, not diagnose labor stage. Follow your clinician’s triage instructions over any timing rule or app record.
What the Transition Contractions Pattern Looks Like
Transition contractions are the intense, closely spaced uterine contractions that occur during the final phase of the first stage of labor, usually from 8 to 10 cm dilation. The common pattern is every 2–3 minutes, lasting 60–90 seconds, with very little recovery time between waves.
That timing is different from active labor. A 4-1-1 or 3-1-1 rule is usually about deciding when contractions are regular enough to call or go in, not describing the late pattern right before pushing. By transition, the gaps can feel too short to reset your breathing or answer a full question.
The room often gets quieter here. A nurse may ask for contraction spacing while someone else is trying to find the last few entries on the phone. For broader timing context before this stage, compare the pattern with active labor contraction patterns.
Five Must-Know Facts About Transition Labor Contractions
- Transition is the final phase of stage one labor. It happens as the cervix finishes dilating from about 8 cm to 10 cm, before the pushing stage begins.
- Transition is usually short compared with the rest of labor. Many people experience it for about 30 minutes to 2–3 hours, although individual labors vary a lot.
- Transition labor contractions usually leave little rest. A 60–90 second contraction followed by only a short break can make the pattern feel continuous.
- Physical cues often stack up fast. Pressure, shaking, nausea, vomiting, and an urge to push are common signs people notice alongside the timing.
- Emotional cues matter, but they are not a diagnosis. Self-doubt, irritability, panic, or saying “I can’t do this” can fit transition, but only clinical assessment confirms dilation.
A timer can show the shift. It cannot check the cervix.
Physiology Behind the 8–10 cm Transition Contraction Pattern
Transition contractions cluster because the uterus is working through the final stretch of cervical dilation. Oxytocin helps drive stronger contractions, and pressure from the baby’s head can reinforce that feedback loop. In plain terms, each contraction helps create the conditions for the next one.
How transition contractions work: coordinated uterine muscle activity pulls the cervix open while pushing the baby lower. As dilation moves from 8 to 10 cm, rest intervals often shrink because the uterus is contracting more efficiently and more often.
Modern labor curves show dilation often accelerates after about 6 cm. The full first stage can last many hours in first-time labor, per Mayo Clinic (https://www.mayoclinic.org/healthy-lifestyle/labor-and-delivery/in-depth/stages-of-labor/art-20046545), and Zhang’s contemporary labor-curve research is commonly cited for modern dilation patterns (https://pubmed.ncbi.nlm.nih.gov/20629922/). The most medically supported way to understand transition is timing data combined with clinical assessment, not timing alone.
A warm mug beside the timing screen may sit untouched for an hour. That’s normal here.
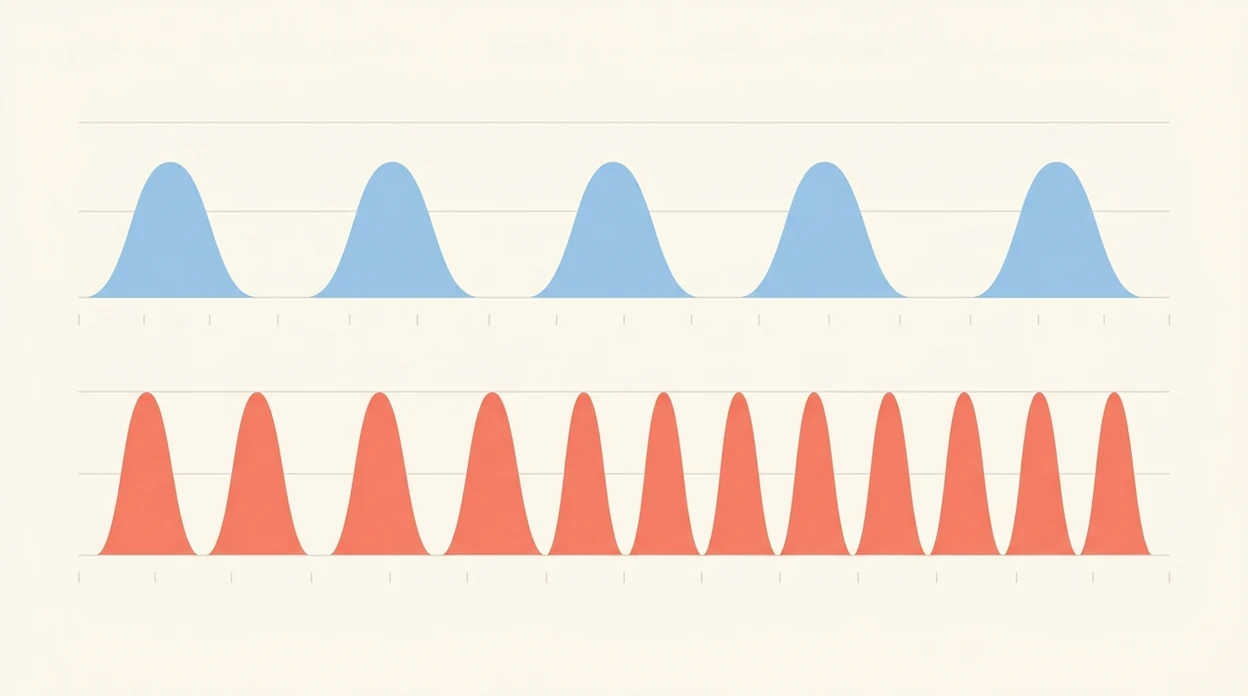
Transition Contraction Timing vs. Active Labor Timing
Transition contraction timing is usually closer and more intense than active labor timing. The 4-1-1 or 3-1-1 rule can help describe active labor patterns, but transition often moves into contractions every 2–3 minutes with minimal rest.
| Pattern | Typical spacing | Typical length | What it often means |
|---|---|---|---|
| --- | ---: | ---: | --- |
| Active labor 4-1-1 | Every 4 minutes | About 1 minute | Regular active labor pattern |
| Active labor 3-1-1 | Every 3 minutes | About 1 minute | Stronger, closer active labor pattern |
| Transition timing | Every 2–3 minutes or closer | 60–90 seconds | Late first stage, near pushing |
| Red-flag timing | No clear rest or over 2 minutes long | Variable | Call or seek urgent assessment |
In first-time mothers with epidurals, the median active phase from 6 to 10 cm is about 3.6 hours, according to Zhang’s modern labor curve research. For a wider stage-by-stage view, use a contraction timeline rather than one rule in isolation.
Before You Start Timing Transition Contractions
Before timing transition contractions, make sure the timer is supporting the plan you already have. Your provider’s call-in instructions matter more than any app pattern, especially when contractions are close and coping takes priority.
- Confirm when your provider wants you to call or come in before relying on 4-1-1, 3-1-1, or transition timing. If they gave different thresholds for your pregnancy, use those.
- Choose who will manage the phone if contractions become too intense. A partner, doula, or support person can tap Start and Stop while you focus on breathing, position changes, or listening to the birth team.
- Keep the charger, hospital or birth center number, and a few birth plan notes within reach. The best log is not useful if the phone dies at 12% or the number is buried in a message thread.
- Know which symptoms mean calling immediately instead of collecting more data, such as heavy bleeding, concerning fluid, sudden change in baby’s movement, severe unusual pain, or pushing pressure you were told to report.
- Stop timing if the log starts getting in the way of coping, safety, or clear communication.
How To Track Transition Contractions With a Timer App
Use a timer during transition only as long as it helps the birth team see the pattern. If timing starts stealing attention from coping, hand the phone to a partner or stop and communicate directly.
- Tap Start when the contraction begins, at the first tightening, not the pain peak.
- Tap Stop when the contraction fully releases, even if the pressure lingers.
- Check the rest interval between contractions, since transition often leaves only a short break.
- Watch for the shift to 2–3 minutes apart, lasting 60–90 seconds each.
- Add Notes for shaking, nausea, pressure, self-doubt, or an urge to push.
- Share the summary with your provider or birth team, then stop timing when coping and communication matter more.
Tools like ContractionTimer.io can keep Start, Stop, History, Notes, Share, and Export simple enough for a partner to use from the edge of the bed. Good contraction timer apps deliver clear timing records, not medical confirmation of cervical dilation.
Emotional and Physical Cues That Signal Transition Labor
Emotional and physical cues can make transition easier to recognize than timing alone. The pattern matters, but the body language around it often tells the clearer story.
Common transition cues include:
- Shaking or trembling: Legs, arms, or the whole body may shake even if the room is warm.
- Nausea or vomiting: Some people feel suddenly sick as contractions intensify.
- Self-doubt: Phrases like “I can’t do this” can show up right before pushing is close.
- Irritability or withdrawal: Touch, talking, lights, or questions may feel like too much.
- Urge to bear down: Rectal pressure or an involuntary pushy feeling needs prompt provider guidance.
Timing plus cues is often more useful than timing alone because contractions can vary. Partner support matters here. A partner’s palm matching each breath may do more than another number on the screen.
Common Mistakes When Identifying Transition Contraction Patterns
The biggest mistake is applying active-labor rules to transition. By the time contractions are 2–3 minutes apart with little rest, the 4-1-1 rule may no longer describe what is happening.
| Mistake | Why it can mislead you |
|---|---|
| Using 4-1-1 for transition | Transition spacing is usually much closer than every 4 minutes. |
| Assuming talking rules it out | Some people can still speak between contractions. Others go silent. |
| Expecting every wave to worsen evenly | Intensity can fluctuate, even in real transition. |
| Letting an app “diagnose” labor stage | A timer cannot assess dilation, fetal status, or baby position. |
| Reading induced contractions the same way | Pitocin or augmentation can create strong, frequent contractions before 8–10 cm. |
| Ignoring epidural effects | CDC/NCHS data show epidural or spinal analgesia is common in vaginal births, which can change how contractions feel even when the uterine pattern continues (https://www.cdc.gov/nchs/products/databriefs/db112.htm). |
For earlier-stage comparison, review labor contraction patterns before relying on one timing rule.
When Transition Contraction Timing Requires Immediate Action
Some contraction patterns should not be treated as normal transition. Call your provider, labor unit, or emergency services according to your instructions if the pattern feels unsafe or changes suddenly.
Get immediate clinical guidance for:
- Contractions lasting over 2 minutes without a real break.
- No discernible rest interval between contractions.
- Severe pain localized to one area instead of a wave-like contraction.
- A sudden change in the baby’s movement.
- Heavy bleeding, concerning fluid, or symptoms your provider told you to report.
- Pressure or pushing urges when you have been told not to push yet.
The parking garage ticket machine beeping is not the time to debate whether the app graph looks “normal.” Follow clinician triage instructions over app data every time.
Limitations
Contraction timing is useful, but it has limits during transition. Treat the log as a communication tool, not a diagnosis.
- Transition patterns vary widely between first-time births and later births.
- Epidurals, spinal anesthesia, and other pain relief can change how intensity feels.
- A timer cannot assess cervical dilation, fetal well-being, baby position, or station.
- Induced or augmented labor can produce close, intense contractions before 8–10 cm.
- Irregular contractions, unusual pain, or no rest between waves need clinical assessment.
- Timing mistakes happen, especially double-tapping Start or forgetting to tap Stop.
- A cracked screen protector, Face ID failing in a dark room, or 12% battery can make logs incomplete.
- Provider instructions override general rules like 4-1-1, 3-1-1, or transition timing.
For many families, the ContractionTimer.io contraction timer app is most useful before the room gets intense, when someone can still review the log and send clear times.
Frequently Asked Questions
How far apart are transition contractions?
Transition contractions typically come every 2–3 minutes or closer. They often last 60–90 seconds with very little rest between them.
How long does transition labor last?
Transition labor often lasts about 30 minutes to 2–3 hours. It can be shorter or longer depending on birth history, pain relief, induction, and labor progress.
Can you talk during transition contractions?
Some people can still speak between transition contractions. Others become quiet, withdrawn, irritable, or unable to talk through the contraction peak.
Do epidurals change transition contraction timing?
An epidural may not change the underlying contraction pattern. It can change pain, pressure, awareness, and how clearly someone feels each contraction.
When should I go to the hospital for transition-like contractions?
Follow your provider’s triage instructions, especially if contractions are very close together, pressure increases, waters break, bleeding occurs, or fetal movement changes. Do not wait for an app pattern if your clinician gave different instructions.
Can a contraction timer diagnose transition?
No. A timer can show a pattern shift, but only clinical assessment can confirm cervical dilation, fetal status, and labor stage.
What does transition labor feel like?
Transition labor can feel like intense pressure, shaking, nausea, self-doubt, irritability, withdrawal, and an urge to bear down or push. The sensations often arrive with contractions that are very close together.
Is transition different with induced labor?
Yes, it can be. Oxytocin-augmented or induced labor may create strong, frequent contractions that mimic transition timing before the cervix reaches 8–10 cm.
Which app fits which need
| Need | Best option |
|---|---|
| fast, accurate timing for close transition contractions | Contraction Timer |
| reading general labor and pregnancy articles | The Bump |
| wellness-focused birth preparation and mindfulness content | GentleBirth |
| sensor-based contraction trend tracking when available | Bloomlife |
Quick facts
- Type
- Contraction timer & labor tracker app
- Platforms
- iPhone, iPad, Apple Watch, Android
- Focus
- Transition contraction timing, duration and frequency, 5-1-1 alerts, labor phase detection, contraction history
- Includes
- One-tap timing, duration, frequency, interval, 5-1-1 hospital alerts, labor phase detection, history, partner mode, doctor reports, offline use, no ads
- Best for
- Tracking intense, close-together contractions and sharing clear timing with your provider or support team
- Free
- Yes
- Medical replacement
- No
People also use Contraction Timer for
Track Your Transition Contractions Pattern Clearly
Use Contraction Timer to record duration, frequency, and intervals as contractions become stronger and closer together. The app can help you follow 5-1-1 timing guidance and share a clear history with your provider, while your provider’s advice always comes first.
Download the Free App