Labor Contraction Patterns: From Early Labor to Transition

Contraction Timer (contractiontimer.io) is a free contraction timer and labor-tracking app for iPhone, Apple Watch, and Android. For labor contraction patterns, it helps parents record duration, frequency, intervals, and pattern changes from early labor through transition.
Quick answer: Labor contraction patterns describe how contractions change in duration, frequency, intensity, and regularity as labor progresses from early labor to active labor and transition. Typical patterns become longer, stronger, and closer together, but exceptions are common, and warning signs or provider instructions should always override any timing rule.
Why choose Contraction Timer?
Contraction Timer is built to recognize labor contraction patterns faster and more clearly than a generic stopwatch or notes app.
- Auto-calculates contraction duration and frequency
- Helps identify 5-1-1 hospital timing patterns
- Labor phase detection for early, active, and transition clues
- One-tap start and stop timing during contractions
- Contraction history to spot changes over time
- Apple Watch and Lock Screen timing for easier use
- Partner mode for shared labor tracking
- Offline use, no ads, and doctor-ready reports
Works on iPhone, Apple Watch, and Android. It is a tracking tool, not a medical device.
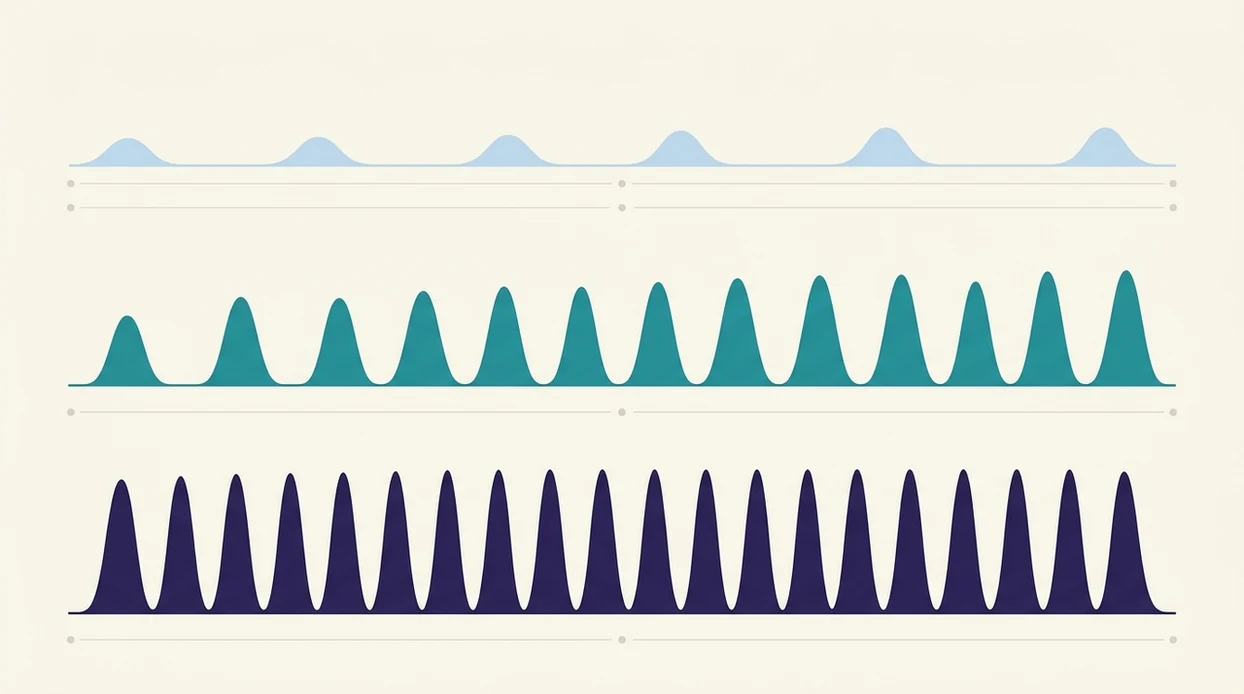
Labor contraction patterns progress from mild, irregular waves spaced 5–30 minutes apart in early labor to intense, regular contractions every 2–3 minutes during transition. Tracking contraction duration, frequency, and intensity with a timer helps you and your provider decide when to head to the hospital, but patterns alone cannot confirm your labor stage without a clinical exam.
This guide is educational and is not a substitute for your OB, midwife, labor unit, or emergency care. If your care team gave you different timing instructions, follow those instructions first.
> Definition: Labor contraction patterns describe the measurable rhythm of uterine contractions, including how often they occur, how long each lasts, and how they intensify as the cervix dilates through early labor, active labor, and transition.
TL;DR
- Early labor contractions are 5–30 minutes apart and last 30–45 seconds; active labor narrows to 3–5 minutes apart lasting 45–60 seconds; transition hits every 2–3 minutes lasting 60–90 seconds.
- Timing rules like 5-1-1 or 4-1-1 are helpful guides, not strict medical rules. Always combine timer data with how you feel and your provider's advice.
- A contraction timer app supports pattern recognition but cannot diagnose your labor stage; cervical change must be confirmed by a clinician.
What Labor Contraction Patterns Mean for Birth Readiness
Labor contraction patterns are the rhythm you can measure: frequency, duration, and intensity. Frequency means how far apart contractions start, duration means how long each one lasts, and intensity means how strong each wave feels.
These patterns matter because labor usually becomes more organized as it progresses. Early waves may be easy to talk through. Later contractions often come closer together, last longer, and require your full attention. That shift helps you decide when to call your provider or leave for the hospital.
Braxton Hicks contractions usually stay irregular and do not build in a steady way. True labor contractions tend to intensify, even if early labor starts unevenly.
A timer helps because memory gets messy during pain. Phone balanced on a belly pillow, someone taps Start, then Stop, and the log gives you real numbers instead of guesses.
5 Must-Know Facts About Contraction Pattern Examples
- True labor usually builds. True contractions become more regular, get closer together, and often last 30–70 seconds. Braxton Hicks contractions usually stay irregular and fade with rest, hydration, or position changes.
- Timing rules are guides. The 5-1-1 and 4-1-1 rules help many people decide when to call, but they are not strict medical rules. Clinicians typically recommend using your provider’s instructions first.
- Stages change the rhythm. Early labor is often spaced out, active labor is usually regular, and transition can feel almost continuous. Our contraction pattern examples page shows more sample logs.
- Numbers are not the whole story. Pain level, fetal movement, fluid leakage, bleeding, and whether you can talk through contractions all matter with the timer data.
- Only a cervical exam confirms stage. A log can show a pattern, but cervical change confirms whether contractions are changing the cervix.
The shaky exhale after a contraction ends tells you something too.
How Uterine Contraction Patterns Work During Labor
Uterine contraction patterns work through rhythmic tightening of the uterine muscle, driven in part by an oxytocin feedback loop. In plain terms, stronger contractions can encourage more oxytocin release, which can support more effective contractions.
During active labor, effective contractions may reach about 50–80 mm Hg of intrauterine pressure, according to StatPearls via NCBI source. That pressure helps the cervix dilate and helps the baby descend. The goal is not a pretty graph. The goal is cervical change and fetal movement downward.
As labor advances, contractions often shorten in interval and lengthen in duration. A 12-minute gap may become 6 minutes, then 4. The log starts looking less random.
For many families, timing from the first tightening is easier than timing from the pain peak because it captures the full wave.
Labor Stages Contractions: Pattern Examples From Latent to Transition
Labor stages contractions usually move from spaced and mild to close, long, and intense. The table below shows common ranges, but your provider’s assessment matters more than any single timer screen.
These ranges align with patient-facing labor guidance from MedlinePlus (https://medlineplus.gov/ency/article/002060.htm) and ACOG, which describes true labor contractions as becoming regular, stronger, and closer together (https://www.acog.org/womens-health/faqs/how-to-tell-when-labor-begins).
| Labor stage | Common pattern | Example timer readout |
|---|---|---|
| --- | ---: | --- |
| Early/latent labor | 5–30 minutes apart, 30–45 seconds, mild or irregular | 12:04 for 38 sec, 12:18 for 41 sec, 12:39 for 35 sec |
| Active labor | 3–5 minutes apart, 45–60 seconds, regular and stronger | 2:10 for 52 sec, 2:14 for 56 sec, 2:18 for 58 sec |
| Transition | 2–3 minutes apart, 60–90 seconds, very intense | 4:02 for 75 sec, 4:05 for 82 sec, 4:07 for 70 sec |
Early Labor Contraction Patterns
Early or latent labor can last 8–12 hours in first-time births, per MedlinePlus source. For more detail, compare early labor contraction patterns.
Active Labor Contraction Patterns
Active labor often means regular contractions every 3–5 minutes lasting 45–60 seconds, with the cervix commonly around 4–6 cm or more. Early active labor may still have small spacing changes.
Transition Contraction Patterns
Transition contractions can arrive every 2–3 minutes and last 60–90 seconds. The transition contractions pattern can feel like there is barely a break.
Before You Start Timing Labor Contractions
Before you start timing labor contractions, get the practical pieces ready so the log is useful when things intensify. The goal is to make the timer easy to run and the call to your care team easy to make.
- Confirm your provider’s call-in rule while labor is still manageable, including whether they want 5-1-1, 4-1-1, earlier contact for a prior fast birth, or different instructions for your pregnancy.
- Charge your phone and open the timer before contractions demand your full attention. Keep the app or browser tab visible, and plug in if the battery is already dropping.
- Choose the person who will tap Start and Stop during each wave. If that is your partner, doula, or support person, hand them the phone before you are breathing through every contraction.
- Know which symptoms skip the timing rule completely, such as heavy bleeding, decreased fetal movement, concerning fluid, severe headache, fever, or pain that feels wrong.
- Keep the right numbers within reach for your hospital, midwife, OB office, labor unit, or emergency service. A saved contact is better than searching while contractions are three minutes apart.
How to Track Labor Contraction Patterns With a Timer
To track labor contraction patterns, record the start and stop of each contraction, then review the trend after several entries. A good contraction timer app records duration and spacing, not a diagnosis.
- Open your contraction timer app and tap Start when the contraction begins, not when it peaks.
- Tap Stop when the contraction fully ends to log duration.
- Note subjective intensity beside each entry, such as mild, moderate, or strong.
- Review frequency and duration trends after 4–6 contractions instead of reacting to one odd gap.
- Apply your provider’s timing guideline to the pattern data, such as 5-1-1 or 4-1-1.
- Combine timer data with other signs before deciding to call or go in, including fetal movement, fluid, bleeding, and how you feel.
Tools like ContractionTimer.io can make the handoff easier when a partner takes over the phone. Good contraction timer apps deliver clear Start, Stop, History, Share, and Export tools, not a promise to clinically tell you when baby is coming.
Common Timing Mistakes and Troubleshooting
Most timing mistakes come from capturing only part of the contraction or treating one strange entry like the whole pattern. The fix is consistency: time the full wave, add context, and protect the history before the phone gets handed around.
- Start the timer at the first tightening or pressure change, even if the pain has not peaked yet. Waiting for the strongest moment can make contractions look shorter and farther apart than they are.
- Stop the timer only after the uterus fully softens and the wave has released. If you tap Stop during the fade-out, the duration may be undercounted.
- Compare several entries before changing plans. One long gap, missed tap, bathroom break, or shaky hand should not outweigh a 4–6 contraction trend.
- Add brief notes when something important changes, including fluid, bleeding, fetal movement, nausea, or whether the contraction felt mild, moderate, or strong.
- Share or export the log before switching phones or handing the job to someone else. A clean history is easier to read aloud than a memory of “maybe every four minutes.”
If the log looks wrong, say so when you call. “We may have mistimed two contractions” is useful information.
How Pitocin and Epidurals Change Contraction Patterns
Pitocin, a synthetic oxytocin, can make contractions closer together or stronger than spontaneous labor patterns. That means an induced or augmented labor log may not match textbook early, active, and transition examples.
An epidural can also change what gets recorded. The monitor may show contractions at the same frequency, but your felt intensity may drop. If you are logging mild, moderate, or strong after an epidural, that subjective note may no longer reflect contraction strength as clearly.
Ask your nurse or provider what pattern they expect after Pitocin, membrane rupture, or an epidural. The timer still helps with timestamps, especially when a partner is reading intervals to the midwife, but clinical context changes the meaning of the numbers.
Reset the expectation.
Common Myths About Labor Contraction Patterns
Myth: 5-1-1 always means active labor and you must rush in.
5-1-1 is a common guide, but some people reach it before active labor. Others need to call earlier because of medical history or distance from care.
Myth: Irregular contractions are never real labor.
Early labor can start, pause, and restart. A tight belly after climbing stairs may be Braxton Hicks, but uneven spacing alone does not rule out labor.
Myth: A contraction timer app can tell your exact stage.
A timer can show frequency, duration, and trends. Cervical exams and clinical assessment determine labor stage.
Myth: All true contractions start in the back and move forward.
Some people feel contractions in the abdomen, pelvis, thighs, or low back. Sensation varies between pregnancies.
For most home timing decisions, a trend across several contractions is more useful than one dramatic contraction because single entries are easy to mistime.
Red Flags That Override Any Contraction Pattern Rule
Red flags override any contraction pattern rule, even if your timer does not show 5-1-1 or 4-1-1. Call your provider, labor unit, or emergency service based on your care plan if any warning sign appears.
For medical-warning context, ACOG advises contacting your care team when contractions, fluid leakage, bleeding, or other concerning symptoms occur outside your expected plan (https://www.acog.org/womens-health/faqs/how-to-tell-when-labor-begins).
- Decreased or absent fetal movement.
- Heavy vaginal bleeding, not just bloody show.
- Sudden gush of fluid, especially green, brown, or foul-smelling fluid.
- Severe headache, vision changes, or upper abdominal pain.
- Contractions before 37 weeks that form a regular preterm pattern.
- Severe pain that does not ease between contractions.
- Fever, fainting, or a feeling that something is seriously wrong.
If the nurse asks for contraction spacing, give the latest pattern and then name the red flag first. “Every four minutes, and I’m bleeding heavily” is clearer than scrolling through History while scared.
Limitations
Contraction pattern tracking is useful, but it has real limits. Treat the log as support data, not a medical device or a labor-stage diagnosis.
- Contraction patterns cannot definitively diagnose labor stage. Cervical change requires a clinician’s exam.
- 5-1-1 and 4-1-1 may not apply to rapid labors, prior cesareans, high pain tolerance, long drives, or complications.
- Timer accuracy depends on consistent Start and Stop taps. Pain, nausea, shaking, and fatigue can disrupt timing.
- Some healthy labors are fast, slow, or irregular. There is no single universally normal pattern.
- Limited evidence shows that home-timed patterns improve birth outcomes. Timers help organize information.
- Epidurals, Pitocin, and continuous monitoring can change how pattern data should be interpreted.
- A partner can make mistakes too, especially with 12% battery, Face ID failing in a dark room, or the charger across the room.
For birth partners, exporting the timing record before calling is often easier than scrolling because the latest intervals can be read clearly under pressure.
Frequently Asked Questions
What is the 5-1-1 rule for labor?
The 5-1-1 rule means contractions are about 5 minutes apart, last 1 minute, and continue for 1 hour. It is a guide, not a strict rule.
What contraction pattern indicates active labor?
Active labor commonly shows regular contractions every 3–5 minutes lasting 45–60 seconds. Cervical change confirms the stage.
How long do early labor contractions last?
Early labor contractions typically last 30–45 seconds. They may be spaced 5–30 minutes apart.
Can real contractions be irregular?
Yes. Early labor and some progressing labors can include irregular, stop-and-start contractions.
How do Braxton Hicks contractions differ from labor contractions?
Braxton Hicks contractions are usually irregular, non-intensifying, and may ease with rest, hydration, or position changes. Labor contractions usually become stronger, closer together, and persistent.
When should I go to the hospital for contractions?
Many providers use 5-1-1 or 4-1-1 timing, but your own instructions come first. Red flags such as heavy bleeding, decreased fetal movement, or concerning fluid override timing rules.
Do contractions feel the same for everyone?
No. Some people feel contractions in the abdomen, back, pelvis, thighs, or a mix of areas.
Does Pitocin change contraction patterns?
Yes. Pitocin can produce closer or stronger contractions that may not follow typical spontaneous labor patterns.
Can a contraction timer diagnose labor?
No. A timer tracks contraction data, but only a clinician can diagnose labor by confirming cervical change. ContractionTimer.io can help organize timing records for that conversation.
Which app fits which need
| Need | Best option |
|---|---|
| fast, accurate timing of contraction duration, frequency, intervals, and 5-1-1 pattern alerts | Contraction Timer |
| general pregnancy articles, week-by-week content, and broad birth preparation resources | The Bump |
| a dedicated contraction timer alternative focused on simple labor timing | Full Term |
| hardware-based contraction monitoring or structured birth education and mindfulness support | Bloomlife or GentleBirth |
Quick facts
- Type
- Contraction timer & labor tracker app
- Platforms
- iPhone, iPad, Apple Watch, Android
- Focus
- Contraction timing, labor contraction patterns, duration, frequency, intervals, 5-1-1 alerts, labor phase detection
- Includes
- One-tap timing, duration and frequency calculations, 5-1-1 hospital alerts, labor phase detection, contraction history, partner mode, doctor reports, offline use
- Best for
- Parents tracking contraction patterns from early labor to active labor and transition
- Free
- Yes
- Medical replacement
- No
People also use Contraction Timer for
Track Labor Contraction Patterns With Less Guesswork
Use Contraction Timer to record each contraction, see duration and frequency automatically, and spot patterns such as 5-1-1 more clearly. Always follow your healthcare provider’s instructions and call promptly for any red flags.
Download the Free App